CLOPIDOGREL – CASE STUDY 1
Updated case report in press
WARFARIN – CASE STUDY 2
Mr V is a 45 year old man with an artificial heart valve. When he started on warfarin it took two weeks for his doctor to find the right dose. Mr V was found to have warfarin resistance, a rare phenomenon, which is genetically determined. This leads to him requiring comparatively high doses of warfarin e.g. >15mg per day. With a genetic test that would have screened for this variant the correct dose may have been prescribed earlier.
A subtherapeutic (low) warfarin response in the early period when starting warfarin is associated with an increased risk of clotting.
STATINS – CASE STUDY 3
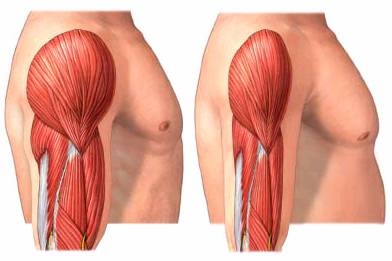
Mrs W. is a 42 year old woman with a liver transplant. She has known coronary artery disease and a total cholesterol of 13 (LDL of 8). She was admitted to hospital with severe rhabdomyolysis (muscle disease) which was thought to be due either to the simvastatin (Lipex) or the transplant medication she was taking. She required kidney dialysis because of the muscle disease. Her simvastatin was stopped and she subsequently had a heart attack. Her clinician ordered a theranostic test which showed that simvastatin was probably not the cause of the muscle disease. Simvastatin was restarted and her total cholesterol dropped by 50%.
Figure 1. Statin myopathy is reported in <1% of people on statins, however muscle symptoms are common. When severe the muscle disease (rhabdomyolysis) can lead to kidney failure and death.